The study aimed to assess the association between Candida species and some dermatophytes in infants with napkin dermatitis and determine the prevalence of DD in relation with yeast (Candida) colonization and identify common Candida spp. which is responsible for Candida (fungal) DD among infants.
Diaper dermatitis (DD) is the most common cutaneous diagnosis in infancy that affects almost every child during the early months of their life time; most cases are associated with the yeast colonization of Candida or DD candidiasis and some dermatophytes. It is an irritating and inflammatory acute dermatitis in the perineal and perianal areas resulting from the occlusion and irritation caused by diapers. The study aimed to assess the association between Candida species and some dermatophytes in infants with napkin dermatitis and determine the prevalence of DD in relation with yeast ( Candida ) colonization and identify common Candida spp. which is responsible for Candida (fungal) DD among infants.
Isolation and Identification of Candida Species and Some Superficial Mycosis Associated with Diaper Dermatitis
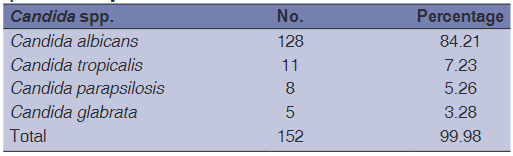
From the total yeast number, Candida albicans was the most predominant species accounting 128 (84.21%), while 24 (15.78%) were non-albicans and dermatophyte molds among which Malassezias spp that accounted 26 (13.83%) and 10 (5.32%), respectively.
Yeast that belongs to the genus Candida can cause both superficial and invasive infections. Superficial infections include oropharyngeal infection or thrush, called yeast infection and diaper rash, fungi in the Candida genus have emerged as major human pathogen, become the fourth leading cause of infection (Harwood, 2013; Ramage et al., 2005). Diaper dermatitis (DD) is one of the most common skin conditions in neonates, infants, and toddlers. Informal observation made in public hospitals reported that approximately four in ten neonates suffer from DD (Shuen, 2015; Pfaller and Diekema, 2007).
Napkin dermatitis (ND), also called DD, diaper rash, and nappy rash. ND is one of the most common skin diseases during infancy and in toddlers (Karsani et al., 2017), which can be associated with different infections, especially Candida infection (Klunk et al., 2014). Other superficial mycotic conditions commonly found in the diaper area are dermatophytosis or tinea infections, exacerbation of seborrheic dermatitis by Malassezia yeasts (Parry et al., 1982; Bonifaz et al., 2016). It is one of the most common disorders in infancy and newborns, accounting for 10–20% of all skin disease (Chiabi et al., 2018). The prevalence in infants has been estimated to be 7%–35% with peak in incidence between ages 9–12 months. Recently however a large scale-study in Great Britain demonstrated an incidence of 25% in first 4 weeks of life alone (Ward et al., 2000).
Studies by Bonifaz et al. (2016), Hoeger et al. (2010), and Spraker et al. (2006) found that Candida albicans is the leading microorganism that causes DD, generally C. albicans occurs in over 70–80% of DD. The origin of these yeasts is directly related to the intestinal flora and they have been isolated in children with oral and esophageal Candidiasis (thrush). The clinical symptoms in these cases are more sever because the yeasts are excreted in the feces (Bonifaz et al., 2016).
A series of factors favor Candida infection in the diaper area. They are mostly acidophilic yeasts that thrive at skin pH, which is around 5.5 or 6.0 in newborns; another proven factor in developing fungi (yeasts and dermatophytes) is CO2 levels, which are higher in the occlusive environment (Odio and Friedlander, 2000; Allen and King, 1978 and Akin et al., 2001). Most reports point out the main infectious agent is C. albicans (80–90%), other species have been found in lesser proportions: Candida tropicalis, Candida parapsilosis, and Candida glabrata (Dan et al., 2006). Candida DD (CDD) is characterized by erythematous and scaly plaques with maceration and edema, sometimes with satellite pustules or papules, the latter being the most characteristic feature of Candida infection. Erosion and ulceration can occur in severe cases (Wolf et al., 2000). The study aimed to determine the colonization of C. albicans (yeast) superficial mycosis in infants with ND.
CANDIDA SPECIES MATERIALS AND METHODS
Sample Collection and Preparation
The study was carried out during the period January 2018 to August 2018. Two hundred and ten infants between 0 and 18 months of age were investigated, the cases selected for the study are all presenting clinical manifestation of DD and suffering from DD, also suggested to be infected with Candida species and non- Candida species. A detailed history has been taken with special reference to predisposing factors. Skin swab and scrapping swabs have been collected from all infants; the swabs then were transported to the laboratory and processed directly.
Swab Specimens from Diaper Area
Clinical presentation was done, samples were carefully scraped from the skin region covered by the diaper for all cases, and four signs were evaluated clinically: Erythema, scaling, maceration, and edema. Swabs carefully labeled and transferred to the laboratory were divided into two smears: One smear was examined immediately under microscope for direct examination and the other usually was cultured on Sabouraud’s Dextrose agar (SDA) medium.
KOH (10%) Direct Examination
One of the swabs taken from the diaper area for direct examination to show mycological elements, should reveal spherical to budding cells, pseudohyphae and blastoconidia pointing to Candida sp., blastoconidia are only found in C. glabrata infection.
Culture
The other swabs was directly inoculated on to SDA with chloramphenicol (0.05 mg/1 m) and cycloheximide (Micromedia, Hungary) and incubated at 25–30c for 2 weeks and examined every 2–3 days, the negative cultures were discarded after 4 weeks, while positive cultures were examined both macroscopically and microscopically for species identification (McGinnis, 1980; Sumathi et al., 2013).
Identification of Fungal Isolates
The mycological identification was based on macroscopic and microscopic examination of the culture isolates. The macroscopic examination of isolated species was characterized by duration of growth, surface morphology and pigment production on the reverse, which based on pigment production on the media (Emmons et al., 1977). The microscopic examination of fungal growth was observed with lactophenol cotton blue stain. Nature of mycelium and conidia formation (macro and micro conidia) helped to differentiate these species (Azab et al., 2012).
Identification of Candida Species from Swabs taken at Diaper Area
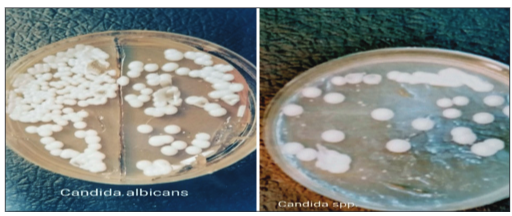
Candida was identified depending on the morphological features on culture medium and germ tube formation as shown in [Figure 1], the identity of other Candida species was confirmed by API test as shown in [Figure 2], based on fermentation, enzyme activity, and formation of hyphae (API-20C Aux: Bio Merieux). Different species had been obtained in current study. Stock culture was made by inoculating single colony of isolated yeast into a slant of SDA.
Figure 1: Colony of Candida albicans and Candida spp. on Sabourauds dextrose agarFigure 3: Microscopic identification of Epidermophyton spp. chlamydoconidia
Germ Tube Test
C. albicans produce true germ tubes (long tube-like projection extending from the yeast cells) when incubated 2 h in serum at 37°C.
Figure 2: API test used for identification of yeast in the present study
Chrom Agar for Identification of Candida
Candida was inoculated in chrom agar and incubated at 37°C for 72 h, for presumptive differentiation of Candida species through color production of colonies due to enzymatic activity.
Dermatophytes Identification
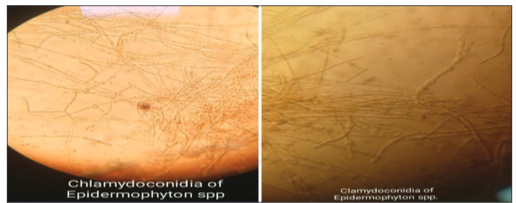
Identification of dermatophyte species was performed by examining the basis of macroscopic and microscopic characteristics of organisms grown in cultures, [Figure 3]. Urease test is used for distinguishing species of Trichophyton spp. (Campbell et al., 2013).
Figure 3: Microscopic identification of Epidermophyton spp. chlamydoconidia
Malassezia Identification
Because its lipophilic yeast was required lipid in the medium for growth, the diagnosis is confirmed by direct microscopic examination of scraping of infected diaper area. Treated with 10–20%KOH, short unbranched hyphae and spherical cells are observed (Bonifaz et al., 2016; Jawetez et al., 1998).
RESULTS
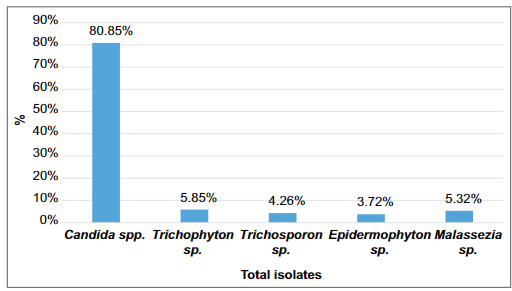
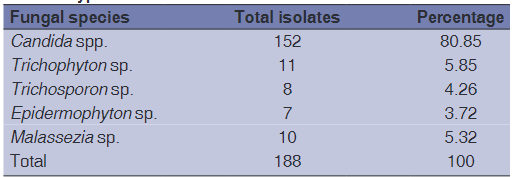
Out of 210 infants with manifestation of clinical DD, 188 (89.52%) cases showed positive cultures for yeast, and dermatophytes. The number and percentage of Candida species, Malassezia spp. and dermatophytes isolated from these cases were, Candida spp. 152 (80.85%), Trichophyton ssp. 11 (5.85%), Trichosporon sp. 8 (4.26%), Epidermophyton spp. 7 (3.72%), and Malassezia spp. 10 (5.32%), as shown in Table 1 and Figure 4 Among the total Candida isolated 128 (84.21%) were C. albicans and the remaining 24 (15.77%) were non-albicans Candida. Among the non albicans 11 (7.23%) were C. tropicalis, 8 (5.26%) were C. parapsilosis, and 5 (3.28%) were C. glabrata, respectively, according Chrom agar results are summarized in Table 2.
Figure 4: The percentage of isolated fungi in the present study
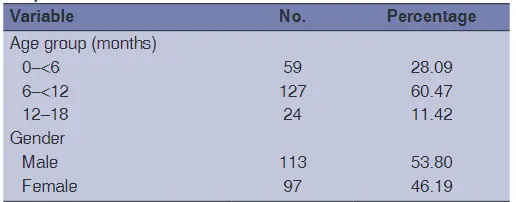
Table 3 shows the most represented age group with DD was 6–<12 months (60.47%) and out of 210 infants with Diaper rash, 53.80% were male and 46.19% were females, it mean high frequency found in males than females.
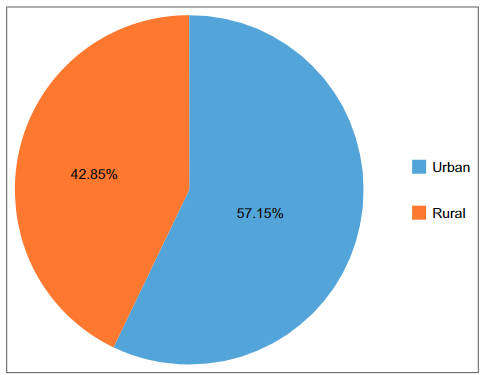
In this study, 57.15% infant with DD resided in Urban areas were 42.85% resided in rural area, as shown in Figure 5.
Figure 5: Area of residence (distribution of infants in rural and urban area)
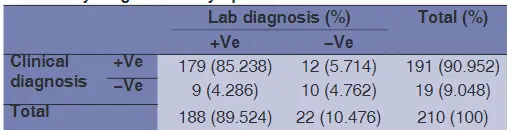
Table 4 compares the efficiency of clinical and laboratory diagnosis of DD, in 210 cases studied, it shows that mistaken occur in 5.71% of symptomatic cases examined, moreover 4.28% with no symptoms, while lab diagnosis is positive which is highly significant.
Table 5 shows the comparison between the diagnosis based on direct smear and that based on cultural technique. Out of 210 infants clinically examined, 188 (89.52%) were positive by both methods, and 22 (10.47%) were negative by both methods.
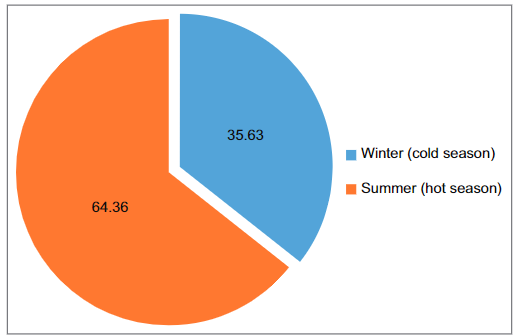
Figure 6 shows that percentages of infants with DD are higher in hot season than cold seasoned were 64.36% and 35.63%, respectively.
Figure 6: Relation of seasons with diaper dermatitis
DISCUSSION
DD can cause significant discomfort for infants and distress for their parents (Seifi et al., 2017). DD can occur any time during infancy (Catherine and Bendel, 2007). Colonization by Candida spp. is significantly more frequent in children with DD than in those with healthy skin (AL-Waili, 2005).
Candidal DD usually presents with beefy, red, and raised edge skin rash with pin pointed satellite lesions, which often extend in to the folds of the skin in the diaper area (Singalavanija and Frieden 1995). Many experts believe that the presence of Candidal infection play a primary as well as secondary role in the development of DD frequently and sometimes painful euroption (Karsani et al., 2017).
The main finding of this study was C. albicans, Malassezia, and some dermatophytes which detected in skin area of diaper, as shown in Table 1, diaper area colonization by Candida species was 152 (80.85%), Malassezia 10 (5.32%), Trichosporo n 8 (4.26%), and dermatophytes 18 (9.57%), respectively, this finding is in concurrence with (Karsani et al., 2017), that improved the main predisposing factors for ND from diaper area include Candid a, this due to that Candida yeast is usually present on skin, especially near genitalia (Piotr, 2014), but when virulence is high they induce a superficial cutaneous candidiasis or come from gastro intestinal colonization, and the moist, warm, occluded skin of diaper area provides an optimal environment for growth, both diarrhea and oral antibiotics
Table 1: Frequency and percentage of fungi isolated from clinical types
Which is similar with the results of this study was C. albicans 128 (84.21%), results in Table 2 showed that the other species of Candid
a was isolated were C. tropicalis 11 (7.23%), C. parapsilosis 8 (5.26%) and C. glabrat a 5 (3.28%) respectively which is similar with results made by (Bendel, 2011), that who isolate C. glabrat a and C. parapsilosis, also similar results showed by researcher (Perween et al., 2019) that they isolates (66.02%) C. albicans and remaining (33.98%) were non-albicans Candid a. Among non-albicans isolated were C. glabrat a 11, C. tropicalis 5, Candida krusei 5, C. parapsilosis 7.3% respectively.
Table 2: Candida spp. isolated from positive cultures in the present study
The previous studies have shown that dermatophyte DD has been studied for many years, the most frequently isolated etiological agent is Epidermophyton floccosum found in around 80% of isolates, followed by Trichophyton rubrum. Furthermore, Malassezia yeasts can aggravate condition affecting the diaper area (Perween et al., 2019). These results are partially agreed with those obtained in this study Trichophyton 5.85%, Epidermophyton 3.72%, and Malassezia 5.31%, respectively. The results of same table showed that
4.25% isolated belongs to Tricophyton spp. which is agree with studies made by (Rafat et al., 2019) that showed the lowest prevalence of Trichosporon isolation is related to infant age group.
Results in this study as shown in Table 3 are similar to these found by Wanjika et al., 2016 in Kenya (Karsani et al., 2017) that infants in the 6 < 12 months age group were predominant with diaper rash and peak of this incidence was 127 (60.47%) cases.
Table 3: Demographic characteristics for the 210 infant with diaper dermatitis
Infants residing in urban areas were the most represented 120 (57.14%) as shown in Figure 5, results in this study are contrary to those of Lietal in 2012 in China who noted that most of infants with DD were from rural areas. Results in Table 4 showed that 12 (5.71%) of cases are negative in lab diagnosis, which is agree with results of (Dixon et al., 1969) that they planned to tack scrapings from lesions directly on to slides for microscopy, but suitable material could not always be obtained, some time because of mildness of the rash but more often because of the presence of ointment which defined attempts at removal or scraping and also demonstrated that some time they thick other dermatological cases but when we direct examined the microorganism occur, were 9 (4.28%).
Table 4: Comparison between the efficiency of clinical and laboratory diagnosis in symptomatic cases studied
The results agree with Karsani et al., 2017, that find certain environmental condition notably elevated temperature and humidity are associated with increased frequency of isolation of C. albicans from diaper area as shown in Figure 6 that in hot season, diaper Candidiasis are higher than cold season, were 121 (64.6%) and 67 (35.63%), respectively.
CONCLUSION
The present study has reported that different Candida species causes DD in infants, but the most predominant isolated was C. albicans , later non- albicans Candida, Malassezia, Trichosporon, and Drmatophytes. CDD was predominant at age group (6–< 12) months. The severity of ND was occurred more in hot seasons than cold season. Furthermore, results concluded that laboratory diagnosis is more efficient than clinical diagnosis because some time related to other dermatological cases.
Credit to: Vian B. Nehmatulla, Department of Basic Science-Microbiology Unit, College of Medicine, Hawler Medical University,